Search
Investigating changes in retinopathy, aortic intima media thickness & heart rate variability, indicators of macrovascular disease & autonomic neuropathy
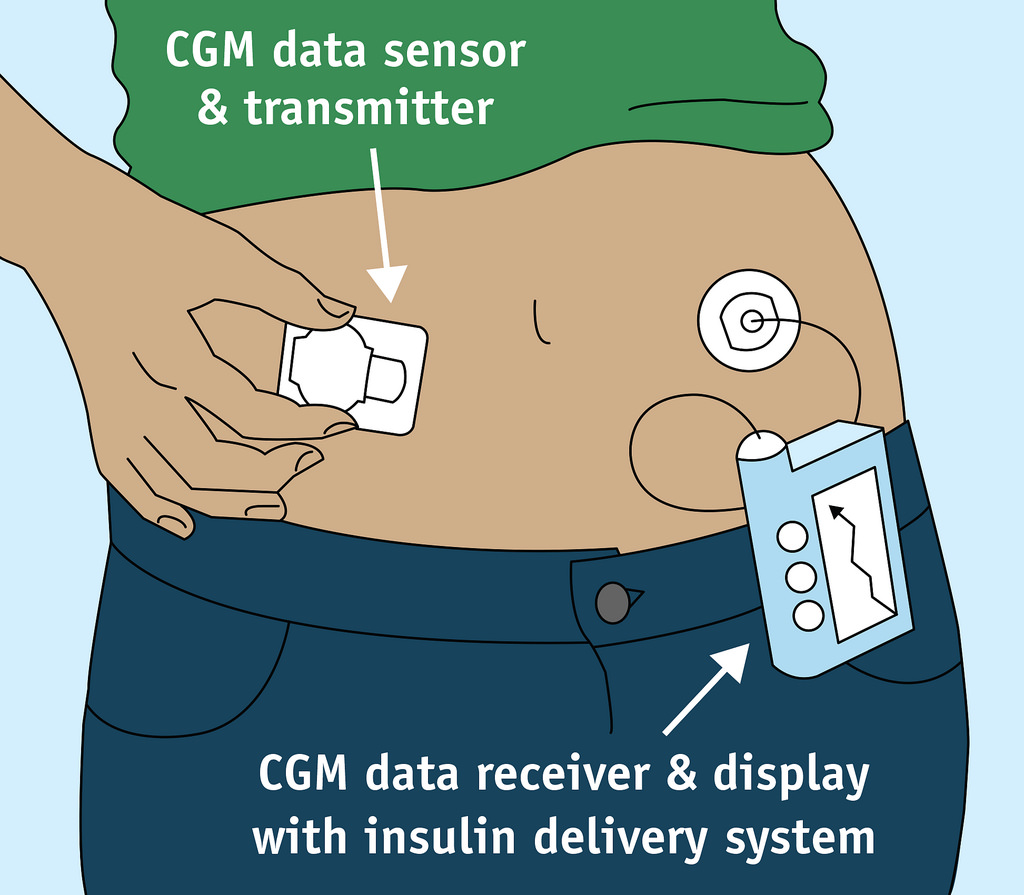
A Closed-Loop System will potentially have a major impact upon acute and chronic complications of diabetes as well as upon their quality of life.
This study will evaluate the effect of two types of aerobic exercise
Determining if hyperglycaemia prior to and during exercise affects the amount of carbohydrate required to maintain stable glucose levels during/after exercise
This study is looking for the causes of type 1 diabetes, so that we can find ways to prevent it.
Investigating the demographic, lifestyle and diabetes management factors associated with the incidence of severe hypoglycemia
The objectives of this study are to study the epidemiology of childhood diabetes in Western Australia from 1985 onwards.
A clinical trial-based economic evaluation was performed in which the net costs and effectiveness of the two treatment modalities were calculated and...
This study analysed spatial and historical variation in childhood incidence of type 1 diabetes mellitus (T1DM) among Western Australia's 36 Health Districts...
Our objective was to determine the separate and combined effects of high-protein (HP) and high-fat (HF) meals, with the same carbohydrate content, on...